
Dispatch #9: How do Indians access and spend on healthcare?
In this dispatch, we analyse the data from the 75th round of the NSS to understand how Indians are accessing and spending on healthcare.

The infant deaths at a government hospital in Kota, in January this year, has once again reminded us of the systemic neglect of public healthcare in India. The factors that scourge India’s state-owned healthcare facilities are infrastructure, poor quality of care and inadequate (or often untrained) manpower. This has resulted in massive levels of distrust towards government healthcare services and providers among the people who, in hordes, are lining up at the private hospitals.
According to the latest NSSO report titled ‘Key indicators of social consumption in India: Health‘, more Indians are accessing private healthcare providers even though the private healthcare services are expensive.
Below are the 11 charts from the report that explains how Indians are accessing and spending on healthcare services.
1) More Indians are accessing private health services than govt or public hospitals.

In the above chart, we can see that the maximum number of ailments are treated either by the private hospital or by a private clinic and private doctor. Government hospitals treat only 32.5% and 26.2% of ailments in rural and urban India respectively. In the absence of doctors and healthcare facilities, 4.3% of the rural respondents go to informal providers. This implies a massive trust deficit towards the public and government hospitals.
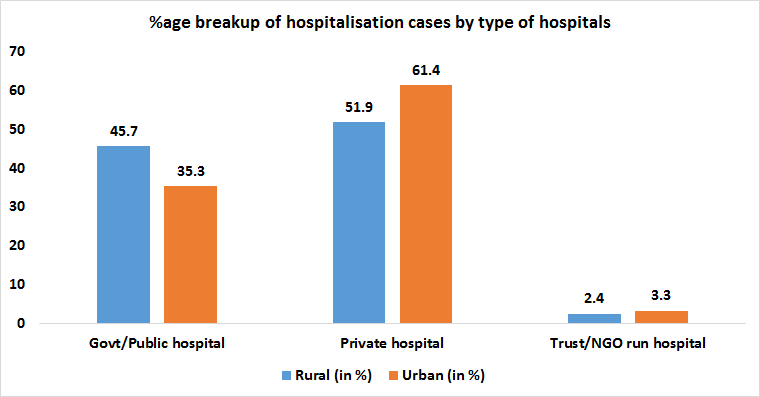
2) The same trend continues in the hospitalisation cases or the cases in which people have to be admitted to the hospital as an in-patient. According to the report, private hospitals corner the maximum number of hospitalisation cases, both in rural and urban India.
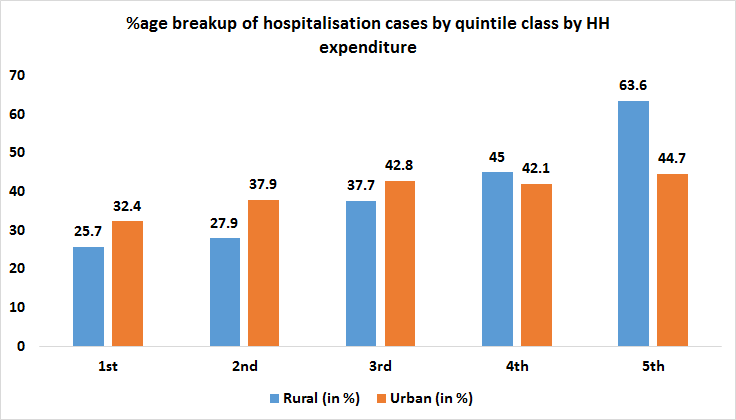
3) Hospitalisation cases in India have a class angle to it. The richer you are, your probability to reach out to hospitals to get yourself admitted for your ailment is higher. The in-patient treatment is costlier than the out-patient treatment because of a hospital bed and other costs. Hence, people from higher-income quintile, both in rural and urban India, access hospitals more than the people from the lower-income quintile.
4) For most of the Indians, the major source for financing hospital expenses is the household savings and income. This arrangement becomes more precarious for people in low-income quintiles since one episode of illness in their family can wipe out most of the household savings. This is what Prof Anirudh Krishna calls the ‘One Illness Away’ phenomenon.

According to the 2017 World Bank report titled ‘Tracking Universal Health Coverage: 2017 Global Monitoring Report’, nearly 5 crore Indians were slipped into poverty in 2011 because of the catastrophic health expenditure. The report, jointly written by the WHO and the WB, suggests that the incidence of impoverishment in India in 2011, due to out-of-pocket health expenditure, was 4.2% (5 crore) if we take $ 1.90 as poverty line and 4.6% (5.6 crore) if we take $ 3.10 as the poverty line.

5) More people have health expenditure coverage in higher-income quintile than in lower-income quintile. This could be because working people who come under government-sponsored health insurance programs like ESIS and CGHS fall in higher-income quintile.
The data, for this particular round of NSSO survey, was collected between July 2017 and June 2018, while the government-sponsored health insurance scheme to cover hospitalisation costs for low-income households, Ayushman Bharat was launched in August 2018. Hence some of these numbers would vary in the present context.

6) Both in rural and urban India, the average medical expenditure per hospitalisation case is way higher in private hospitals than in government hospitals. This is like a double whammy for people seeking treatment. On the one hand, we have a crippling public health system, on the other hand, we have a private health system that offers health services but at very high costs. As a result, people access private hospitals and care providers more than the public ones even though they are costly. And since the coverage of any kind of health insurance is low, the out-of-pocket expenditure for any illness episode for Indians is high.

7) Cancer is slowly emerging as one of the biggest killers in India. Every day nearly 2100 Indians die due to cancer. The treatment of cancer, according to the NSSO data, is the costliest one, both in government and in a private hospital. While the average medical expenditure for cancer cases in a public hospital is Rs. 22,520, the average medical expenditure in a private hospital is Rs. 93,305. This is too big an amount for people in middle and low-income quintiles.

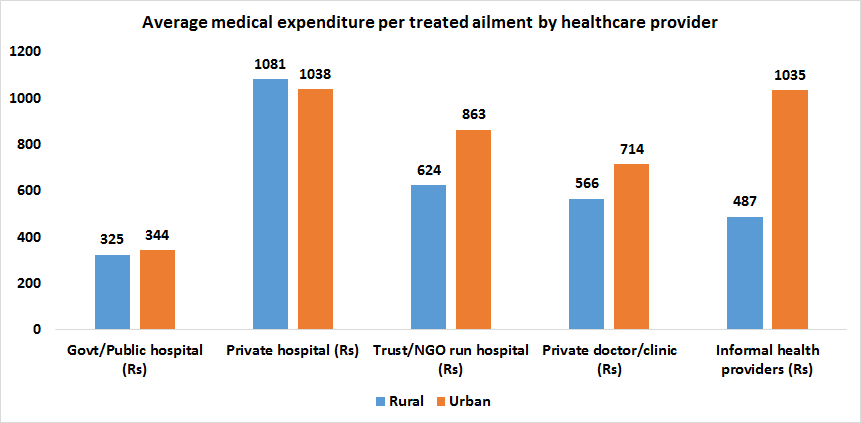
8) The average medical expenditure per treated ailment is being incurred more by the private hospital and private clinic and doctor. Equally costly is getting aliment treated by informal health providers.
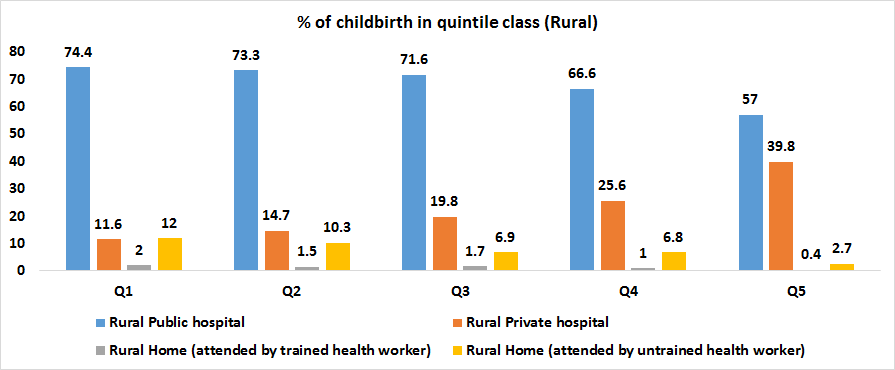
9) Stories of infant deaths come mostly from government hospitals. This is because a large proportion of rural India goes to the government hospitals and health centres for childbirth as compared to urban India.
Within rural India, the dependence on government hospitals for childbirth is high across all the income quintile class. The share of private hospital increases only after the 4th income quintile. This implies that the rich in rural areas are tend to go to private hospitals for childbirth as compared to the rural poor.
10) The trend in urban India is very different from that in rural India. In urban areas, as the incomes increase people’s access to private hospitals increases while access to government hospitals decreases. This clearly indicates that in urban areas, the rich have given up on government hospitals and rely on private hospitals. The people from low-income quintiles have no other choice but to go to public hospitals for the childbirth.
And with poor quality of care, abysmal infrastructure and inadequate staff, the poor always get poor services in government and public hospitals.

11) Childbirth is more costly in private hospitals than in public hospitals. The average expenditure on hospital childbirth is almost double in private hospitals than in public hospitals in both rural and urban areas.

12) The social group which an Indian belongs to determine the likelihood of the childbirth happening in a private hospital which is costly as compared to a public hospital where the quality of care is poor. In both urban and rural areas, a higher percentage of SCs and STs access public hospitals as compared to private hospitals for childbirth.

Access to hospital care:
In the latest EPW issue, Imrana Qadeer and Sourindra Mohan Ghosh, have analysed the data from the National Sample Survey 75th round report and the National Health Profile to compare the utilization of public and private hospitals. The two assumptions taken by the authors are that a) the states having a low vacancy of hospital beds in public hospitals indicate a shortage of beds and b) the states having a high vacancy of hospital beds in public hospitals indicate accessibility, availability or poor quality of care in public hospitals. They created a 2x2 grid with four quadrants. On the x-axis, we have vacant public hospital beds in percentage and on the y-axis we have a percentage of occupied beds in private hospitals.

Each quadrant represents a different group of states:
1) Group A (Maharashtra, Telangana, Uttarakhand, UP, Gujarat, Haryana, Punjab, Karnataka)- These states have a high vacancy of beds in public hospitals and a high percentage of occupancy of beds in private hospitals. This clearly indicates the availability, accessibility and poor care quality issues in public hospitals.
2) Group B (AP, Chhattisgarh, Kerala, Bihar)- These states have a low vacancy of beds in public hospitals and a high share of hospitalisation in private hospitals. This clearly indicates the shortage of beds in public health facilities. The authors claim that Bihar is an extreme case with acute shortage of public hospital beds (only 10% are vacant) and significant use of private hospital beds.
3) Group C (Odisha, MP, WB, J&K)- These states have a low vacancy of beds in public hospitals and a low share of beds in private hospitals. This indicates a shortage of beds in the public health facilities and also low penetration of private hospitals. The authors add that only 6% of Odisha’s public hospital beds are vacant and the share of private sector beds in total occupied beds is 33%, indicating low access to private sector hospitals along with grossly insufficient beds in public hospitals.
4) Group D (Jharkhand, TN, Delhi, Rajasthan, Assam, HP)- These states have a high vacancy in public hospitals and also a low occupancy of private hospital beds. These are richer state and hence the authors argue that they have higher access to public hospitals and hence fewer people go to private hospitals.
The authors lament the neglect of public health in terms of per capita expenditure on key public health components like prevention and control of diseases, drug control and food safety.

Per capita expenditure in the selected states under this extremely crucial component is negligible, except for Kerala, which has increased manifold in recent years. Funding on drug control, food safety, public health laboratories, public health education, etc, are also crucial public health components, which—except for Kerala—virtually finds no funding in per capita terms.
-Imrana Qadeer and Sourindra Mohan Ghosh, ‘Public good perspective of public health’, EPW
Good Reads:
1) Public health as a public good- Building on the classical definition of public goods, public health is a collective property that depends principally on the conditions that create public health (i.e. the structural, social, and political forces that produce health of populations) rather than on any individual action. These conditions are features of social structures that are not owned and not buyable by individuals. Salutogenic urban environments seek to be both non-excludable and non-rivalrous; so do policies that incentivize healthier foods and efforts to minimize pollution. As well articulated in Global Public Goods for Health, the provision of public health is inextricably linked to government action and other classic public goods. Therefore, the conditions that promote the health of the public are classic public goods, even if an increasingly assertive ownership society may threaten some of that. Knowledge (for example, on health risks), technology, policy, and health systems have many properties of considered public goods— but, as Smith argues, modern health technologies are “increasingly patented and thus made artificially excludable.” Likewise, health systems, absent public financing, are not affordable to many.
2) How India can lead the world to build a functioning public health system? The world has not yet invested in a cadre of trustworthy, community-embedded public health workers who are empowered to undertake their tasks as professionals, despite the lessons from Ebola virus disease. This article, by Stuti Khemani, provides novel evidence from a survey of public health workers in Bihar that can immediately be used to design a new type of contract with public health workers based on job security, steady wages, and trust in professional norms.
.